Rotator cuff tears are a common cause of shoulder pain and disability. While most tears are due chronic wear in middle-aged and older patients, they can also be caused by trauma in younger patients. Patients usually complain of shoulder pain to the top and side of their shoulder and report difficulty with overhead activities. The rotator cuff functions to provide stability for the shoulder as it is moved throughout it’s wide range of motion by the other muscles of the shoulder. Any disruption to the tendon can cause significant weakness and pain due to altered biomechanics of the shoulder. For partial thickness tears or inflamed tendons, non-operative treatments such as anti-inflammatory medication, injection and therapy can provide good long term improvement.
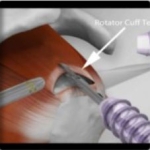
Rotator Cuff Tear
However once a rotator cuff tear becomes full thickness where the tendon is no longer attached to the bone, surgery is typically the best option. Because of the already chronic wear of the tendon and the constant pull on the tear, full thickness tears do not heal by themselves. In fact there is a higher likelihood of worsening of the tear due to increased stress on the remaining portions of the tendon that are still intact, just like a tear in a seam in a piece of clothing. Shoulders with chronic tears that are untreated have a higher likelihood of developing arthritis (figure 3).
Surgery Overview
The surgery to repair the rotator cuff is done arthroscopically. This is less invasive as it preserves the surrounding muscle, which allows earlier return of motion and is usually associated with less post operative pain than an open incision. Arthroscopy also provides better visualization of the shoulder and allows the surgeon to address other injuries in the shoulder such as labral tear, biceps tendinitis, acromioclavicular joint arthritis. The goal of surgery is to reestablish the tendon attachment to the bone and restore the normal biomechanical function of the rotator cuff tendon. This is typically done as an outpatient procedure with 3 small incisions in the shoulder for the camera and instruments (Figure 1 and 2). Patient are typically placed under general anesthesia and also given a regional anesthetic which numbs the shoulder and arm for post operative pain control.
After surgery, patients are placed in a sling for comfort. Immediately after surgery, they are allowed to do light daily activities such as typing, using eating and writing utensils. Driving is allowed once patients no longer need narcotics for pain control. Heavy lifting beyond 5 pounds is not allowed until at least 2 months after surgery to allow for adequate tendon healing. Patients are allowed to do some limited lifting immediately post op as long as it is done with the elbow against the body (eg. pulling levers, assembly on a work bench etc.) Return to full activities or sports usually takes 6 months; however patient may take upwards of 9 month to a year to fully regain strength and function of their shoulder.